

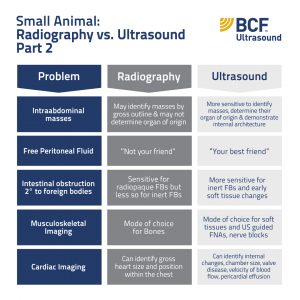
For diagnosing SI obstruction in vomiting dogs, in 2011, Sharma et al. concluded “both abdominal radiography and abdominal ultrasonography are accurate for diagnosing small-intestinal obstruction in vomiting dogs and either may be used depending on availability and examiner choice. Abdominal ultrasonography had greater accuracy, fewer equivocal results and provided greater diagnostic confidence compared with radiography”.
Abdominal radiography is sensitive for detection of radiopaque FBs such as bone, glass, razors, tennis balls, batteries, sand and mineralised or metal objects. However, when inert FBs are suspected such as linear FBs, corn cobs, fruit stones, plastic toys etc, we have to look for subtle soft tissue changes secondary to obstructive disease (ie focal intestinal dilation and/or tear drop gas pattern as evidence of plication), that may not be obvious until late in the course of disease when there is significant pathology present.
Ultrasound is usually more sensitive for detecting those FBs that are radiolucent and often earlier in the clinical course, provided that the sonographer does a thorough exam of the intestinal tract and there is a partial or complete obstruction present. Nowadays, depending on the level of skill of the sonographer, an abdominal ultrasound exam often takes the place of a contrast radiographic GIT study to diagnose gastrointestinal obstructive disease as an underlying cause of vomiting. And if you get a diagnosis on ultrasound without contrast rads you won’t have to deal with regurgitation or intra-abdominal leakage of contrast medium during surgery either.
Ultrasound is a live modality so also better for assessing gut motility or the lack there of in cases of ileus. Don’t forget that in addition to foreign body obstruction, mechanical ileus may also be caused by neoplasia or an intussusception (both of which may be more easily detected on ultrasound). Ideally radiography and ultrasonography should both be employed to investigate suspected cases of foreign body obstruction as they are complimentary.
Ultrasound Tips:
Ultrasonographic features of intestinal foreign bodies may include:
An intraluminal object with a highly attenuating, bright, hyperechoic interface.
Strong distal acoustic shadowing that obscures detail of the intestinal wall in the far-field.
The size, shape and echogenicity will vary depending on the size and shape of foreign body but the more typical patterns are:
Linear FBs usually have a straight hyperechoic line within a loop of intestine and may be anchored in the stomach/pylorus +/- plication of intestine (bunched up, asymmetrical undulation of intestinal walls)
Balls have a smooth, usually curvilinear interface.
Corncobs have a classic irregular interface +/- small curved hyperechoic gas pockets (created by the corn kernels).
Fragments of balls and plastic toys may produce an irregular hyperechoic interface with acoustic shadowing.
Soft rubber balls may allow sound penetration that allows visualisation of the majority of the object sitting within the lumen.
Hairballs and matted hair ties (common in cats) may cause masses of mixed echogenicity with variable shadowing.
 US image of plicated intestines in a MN Beagle secondary to a linear foreign body with anechoic fluid (with some hyperechoic intestinal contents) pooling in a loop orad to the obstruction.
US image of plicated intestines in a MN Beagle secondary to a linear foreign body with anechoic fluid (with some hyperechoic intestinal contents) pooling in a loop orad to the obstruction.
NB: If you see evidence of a linear FB don’t forget to examine the stomach/pylorus and under the tongue for an anchor point!
Additional ultrasonographic features of gastrointestinal obstruction (secondary to FBs):
There may be distention or dilation of the intestine with fluid or gas accumulation proximal to the FB and/or an abrupt narrowing post-obstruction.
There may be fluid accumulation in the stomach and pyloric outflow obstruction secondary to a more distal intestinal obstruction.
Occasionally linear FBs may cause intussusceptions (typical target lesion in transverse view).
There may thickened loops of intestine +/- free abdominal fluid (peritonitis) secondary to inflammation.
There may be free peritoneal gas secondary to intestinal perforation from a FB or intestinal necrosis (radiography is better suited to identifying this).
Abdominal lymph nodes may be enlarged.
Happy scanning… and if you get clear ultrasound images of some interesting foreign bodies please be sure to send us some pics!
































